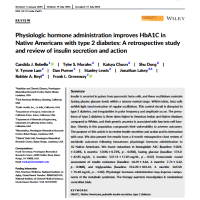
1 A1C - Blood Pressure - Retrospective Study - 67 person - Mercer University School of Medicine - 2022-min
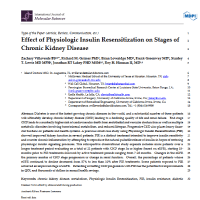
2 Kidney Disease - 17 people - IJMS -2024-min
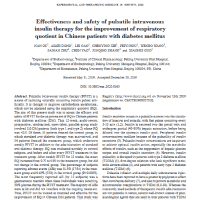
3 Chinese study - Respiratory Quotient - 107 person - 2019-min
4 Retrospective study - 80 patients - IRB - Frontiers in Public Health - 2021-min

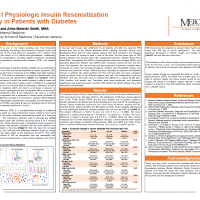
5 Reduced Hospital and ER Visits - Retrospective Study - 1524 patients - Journal of DIabetes, Metabolic Disorders & Control - 2017-min

6 IIIT - Research - Type 1 Diabetes - LANCET - Aoki -1993-min

6.1 Retinopathy - Journal of Diabetes - 2 patients-min

6.2 Kidney Disease - Review - Diabetes Journal-min
6.3 Kidney Function - Review - 3 people - Lakey-min

6.4 HOMA-IR - Fortune Journals - 4 people-min

6.5 Neuropathy Reversal - Study - 2 people - International Journal of Diabetes & Metabolic Disorders - Lakey-min

6.6 Diabetes Complications - ELSEVIER - Research - PIVIT - FIT - 2009-min

7.1 Detailed Review - Medical and Clinical Research - 2021 - Lakey-min
7.2 Research - ELSEVIER - 2019 - Lakey-min

7.3 Review - International Journal of Diabetes & Metabolic Syndrome - Lakey-min
8 Medical policy - CIIIT - 2001-min
9 Insulin Resistance - Reason for MRT - Lakey - International Journal of Molecular Sciences - 2022-min
9.1 Beta cell function - Research - Reason for MRT - Mayfield - 2004-min
9.2 Abstract - Pulsatile Nature of Beta Cells - Upsala Journal of Medical Sciences - 2009-min
9.3 Rationale and Methodology - Pulsatile Nature of Beta Cells - PubMed - 2021-min
9.4 Type 2 Diabetes - Opinion - International Journal of Molecular Sciences - 2022-min
9.5 PIVIT for Out of Control Diabetes - Abstract of Study - Journal of Infusion Nursing - 1995-min